
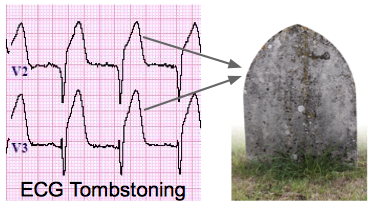
ECG tombstoning is a term for ventricular fibrillation (VF) that occurs in the first few minutes after an acute myocardial infarction (AMI). It is typically seen in the setting of ST-elevation myocardial infarction (STEMI). The following are some possible causes of ECG tombstoning:
Lack of reperfusion therapy: If you have STEMI, you should receive reperfusion therapy as soon as possible. But if you don’t receive this therapy, your risk of developing ECG tombstoning increases significantly.
Toxic levels of potassium: Potassium can accumulate in your body when you have heart failure or kidney disease. This can lead to hyperkalemia — a condition characterized by abnormally high levels of potassium in your blood. Hyperkalemia can cause abnormal heart rhythms and even death if left untreated.
Bradycardia: Bradycardia refers to a slow heart rate below 60 beats per minute. Bradycardia can be caused by various factors such as exercise or stress — but it’s also common after surgery or trauma.
ECG tombstoning is the phenomenon that occurs when a patient has an ECG taken at one time, and then is seen again several hours later with a new ECG. The new ECG will be completely different, even though the patient hasn’t changed position or had anything to eat or drink.
The most common reason for this is lead reversal. The ECG leads are attached to the body in specific positions; however, if they are incorrectly positioned on the body, the electrical signals will be inverted (e.g., V1 will become a negative waveform). This can happen if someone accidentally puts the leads on upside down, or if there is an error in the printing of a report.
The most common cause of lead reversal is when someone attaches electrodes to themselves incorrectly (e.g., attaching a G electrode to an A electrode).
What does tombstoning mean on ECG?
In this post, we will discuss what tombstoning means on ECG. Tombstoning refers to a type of ST elevation in which the ST segment descends below baseline, then returns to baseline as the T wave rises. This pattern can be seen in both acute myocardial infarction and pericarditis.
Tombstoning may be seen in acute myocardial infarction (AMI) with right ventricular involvement or inferior wall AMI. In these cases, the ST segment descends below baseline as it goes through the QRS complex and then returns to baseline as the T wave rises. The reason is that when there is a large area of ischemic tissue within the heart, blood flow must pass through this area before getting to other parts of the heart. As this happens, there is an increase in local afterload which causes a rise in left ventricular pressure which stretches out the myocytes and causes them to activate prematurely (before their time). This premature activation causes an ST segment depression as well as an abnormal T wave morphology that looks like a “camel hump” or “horseshoe” shape on your EKG monitor.
Tombstoning is a term used in electrocardiography to describe the appearance of the ST segment on an electrocardiogram, when the heart is beating normally.
The ST segment is the flat portion of the ECG that occurs between two waves (known as QRS complexes), which represent depolarisation of the ventricles.
When an ECG is obtained, an electrical signal is sent through the body and picked up by electrodes placed on various parts of the body. The shape of this signal reflects what is happening with each heart beat.
Tombstoning can be seen when there is some degree of scarring in the heart muscle after a heart attack or myocardial infarction, where part of the muscle has died. This means that during each heartbeat, only part of the muscle contracts effectively, leaving another part still contracted from previous beats. This results in a partial mismatch between contraction and relaxation phases within each cycle (systole) and leads to a characteristic pattern on an ECG known as tombstoning.”
What does a tombstone ECG look like?
A tombstone ECG is a type of ECG that is used to determine the cause of cardiac arrest. It consists of 12 leads and takes approximately 10 minutes to complete.
The tombstone ECG was developed in the 1980s by Dr. James Beckman at Sinai Hospital in Baltimore, Maryland, United States. The name comes from its resemblance to an old-fashioned tombstone.
The tombstone ECG is used as a diagnostic tool when someone suffers from sudden cardiac arrest (SCA), which can lead to sudden death if not treated quickly. It provides information about the heart’s electrical activity, allowing doctors to diagnose what caused the SCA in the first place and determine whether it’s safe for the patient to receive treatment.
The tombstone ECG is a type of tracing that is used in cardiac arrest. It is also known as a ‘tall’ or ‘high’ peaked T wave.
It is a sign of an acute myocardial infarction (AMI) and represents the final stage of an evolving process where there has been occlusion of a coronary artery followed by reperfusion and reperfusion injury.
The tombstone ECG can occur in any lead but is most commonly seen in V2 or V3. Most patients with tombstone ECGs have had an anterior wall AMI.
The tombstone ECG can be caused by:
acute myocardial infarction (AMI) prior to defibrillation
early repolarisation (ER)
What is V4 V6 in ECG?
A normal sinus rhythm is one of the most common types of ECG waveforms. It has a regular rate and rhythm, with the P wave, QRS complex and T wave all appearing in a predictable pattern.
The P wave represents atrial depolarisation and precedes every QRS complex on the ECG by one small box (approximately 0.04 seconds). The QRS complex represents ventricular depolarisation and occurs within two small boxes following the P wave (approximately 0.1 seconds). The T wave represents ventricular repolarisation and follows the QRS complex by one small box (0.04 seconds).
V4-V6 refers to a segment of the heart’s electrical activity represented by four leads in a quadrant from V4 to V6 (in this case, II, III, aVL and aVR), which you may also see referred to as “extras”.
V4 is the fourth lead in a 12-lead ECG. It is also known as V4R, which stands for “ventricular lead 4 right arm”.
V4 is a relatively new lead that was added to the standard 12-lead ECG. It can be used to diagnose some electrical abnormalities.
V4 is located approximately 1 inch below the right nipple, overlying the intercostal space between the 3rd and 4th ribs. The electrode placement is identical to that of V3, except it’s moved down one rib space and over one intercostal space.
V6 is the sixth lead in a 12-lead ECG. It is also known as V6R, which stands for “ventricular lead 6 right arm”.
V6 can be used to monitor electrical activity in the heart during surgery or other procedures when an implantable cardiac pacemaker (ICP) has been placed in order to make sure it’s working properly and delivering pacing pulses at appropriate times.
The V4-V6 leads are used to measure the electrical activity of the heart. They are a set of leads placed on the right side of the chest, just below the clavicle, and on top of the two upper ribs.
The V4-V6 leads measure the electrical activity coming from ventricular depolarization (the pumping chambers).
What does MI look like on ECG?
The electrocardiogram (ECG) is the most effective investigation that is used to diagnose myocardial infarction (MI). The ECG will show a change in the electrical activity of the heart that occurs as a result of myocardial ischaemia.
What do you need to know about MI?
Myocardial infarction (MI) occurs when there is an obstruction of blood flow to the heart muscle, usually due to plaque rupture or thrombus formation in one of the coronary arteries. These events lead to myocardial cell death and subsequent scar formation within the affected area of the heart wall.
There are two main types of MI: ST elevation MI (STEMI) and non-ST elevation MI (NSTEMI).
ST elevation MI occurs when there are ST changes present on an ECG within 12 hours of symptom onset. This type of MI requires immediate treatment with thrombolysis or primary angioplasty to open up the blocked artery so that blood flow can be restored to the affected area of heart muscle.
NSTEMI occurs when there are no ST changes on an ECG but there are elevated cardiac enzymes (CKMB or troponin) indicating extensive damage within the heart muscle. This
MI is the medical term for a heart attack. It occurs when a blood vessel supplying oxygen and nutrients to the heart muscle is partially or completely blocked. The lack of oxygen causes muscle damage and can lead to heart failure.
The most common symptom of MI is chest pain or discomfort. Other symptoms include:
Pain in your neck, jaw, back or arms
Nausea and vomiting
Shortness of breath
Sweating or paleness
The most common ECG changes are:
ST segment elevation. The ST segment is the flat part of the ECG between the end of one heartbeat and the beginning of the next. During an MI, this area may become elevated, meaning it goes above the baseline level.
Q waves. Q waves are small dips in the ST segment that appear after a certain number of heartbeats (usually three). They represent damage to the heart muscle itself, which can occur as a result of an MI.
T wave inversion. When T waves invert, they flip from being upright to being horizontal (or even negative). In other words, they “fall down” on either side of their baseline position during an MI.
What is abnormal ECG?
What is Abnormal ECG?
Abnormal ECG is defined as any deviation from the normal ECG. There are many causes of abnormal ECGs, and they can be grouped into two categories: 1) artifact, and 2) true pathologic changes. Artifact is any irregularity that is related to technical factors such as poor electrode placement or movement during the exam. True pathologic changes are abnormalities that represent some type of disease process that is occurring in the heart.
Artifactual changes are often seen with ST segment depression (STSD). This occurs when the heart lies posteriorly within the chest cavity. When this happens, there is less blood supply to the heart than usual, which causes it to beat more slowly than normal. This slowing down results in a depressed ST segment on the ECG tracing. The most common cause of this type of STSD is sleep apnea, which can result in significant fatigue after waking up in the morning because your body has not had enough oxygen during sleep due to breathing problems during sleep. Other causes include pulmonary embolism (PE), left ventricular hypertrophy (LVH), hypothyroidism, pericarditis, myocardial infarction (MI), and postural orthostatic t
Abnormal ECG, or electrocardiogram, is a test that measures the electrical activity of your heart.
The test is painless and noninvasive and is usually performed in a doctor’s office or clinic.
The abnormal ECG may be used to diagnose a variety of conditions, including:
Heart attack (myocardial infarction)
Heart rhythm problems, such as atrial fibrillation (AFib) and ventricular arrhythmias (VAs)
Heart valve problems, such as mitral valve prolapse
Abnormal ECG is an ECG with non-specific changes, which can be caused by any number of conditions.
Abnormal ECG can be caused by:
coronary artery disease (CAD)
peripheral vascular disease (PVD)
hyperkalaemia and/or hypokalaemia
Hyperkalaemia is one of the most common causes of abnormal ECG. The reason for this is that hyperkalaemia increases the resting membrane potential by decreasing sodium permeability and increasing potassium permeability. This results in repolarisation abnormalities such as tall T waves, inverted T waves and QT prolongation.
Hypokalaemia also has a significant effect on the resting membrane potential but through a different mechanism. It decreases sodium permeability resulting in hyperpolarisation and therefore shortened QRS duration, ST segment depression and T wave flattening or inversion.
What test confirms an MI?
The most reliable method for confirming an MI is with a cardiac enzyme test, which measures the level of enzymes in the blood. Enzymes are proteins that speed up reactions in the body.
The most common enzyme used to detect an MI is myoglobin (MY-oh-glow-bin). Myoglobin is normally found in muscle tissue and its levels increase when tissue damage occurs.
In some cases, doctors will prescribe other tests that can help confirm an MI, including:
Electrocardiogram (ECG or EKG) – An electrocardiogram shows how well your heart is pumping blood through your heart and how fast it’s beating. If you’re having a heart attack, your heart may not be able to send enough blood out through your arteries to the rest of your body. This can cause low blood pressure and make your heart beat irregularly or very fast. An ECG can help identify these changes and confirm that you’re having a heart attack.
If a patient’s symptoms are suggestive of MI, the doctor will order an electrocardiogram (ECG) to look for changes in the heart’s electrical activity. An ECG is a simple and noninvasive test that records the electrical signals generated by the heart during each heartbeat. Sometimes it detects signs of an MI before other tests do.
The test results can show whether there’s been an MI or not. If there has been, it tells doctors which artery(s) are blocked and what stage of MI it is — ST elevation or Q wave — so they can decide on appropriate treatment.
A heart attack is caused by a sudden blockage of an artery that supplies oxygen to the heart muscle. This can be due to a clot forming in an artery, or it can be due to plaque building up on the artery wall. Either way, if enough of the heart tissue doesn’t receive oxygen, then it will die. This is called myocardial infarction (MI), which is commonly known as a heart attack.
There are two main types of tests that are used to confirm whether someone has had a heart attack:
An ECG monitors the electrical activity of your heart. It records how fast your heart is beating and whether there are any abnormal rhythms that may indicate damage to your heart muscle. It also measures how much oxygen is being supplied to different parts of your heart as this can identify if there is any damage from lack of blood flow.
A CT scan uses X-rays to look at the structure and function of your organs and tissues inside the body. A CT angiogram combines CT scanning with an injection of dye (contrast medium) into a vein which highlights blood vessels on screen — this can show any narrowing or blockages affecting blood flow through arteries and veins within the body’s organs and tissues.”
Do Q waves indicate MI?

Q waves are a sign of myocardial ischemia, or heart attack. Q waves can occur in the absence of MI because of other reasons such as left ventricular hypertrophy. The main difference between LVAH and MI is that LVAH usually occurs without chest pain, while MI usually causes chest pain.
Yes, Q waves are a sign of myocardial infarction (MI).
A Q wave is a negative deflection on an electrocardiogram (ECG) tracing that represents a localized abnormality in the electrical activity of the heart.
In contrast, R waves are positive deflections on an ECGs tracing. The QRS complex is a combination of Q and R waves.,
Q waves are an important indicator of a heart attack. Q waves are often seen in premature ventricular contractions (PVCs). However, they can also be seen following a myocardial infarction (MI).
Q waves can be seen in many conditions, including:
Heart attack
Heart failure
Prolonged QT syndrome
What cardiac markers rule out an MI?
Cardiac markers rule out an MI
I’ve been having chest pain for a few days. I am going to the doctor tomorrow but I wanted to know if cardiac markers could rule out an MI? I don’t want to waste any time getting checked out if it’s nothing serious.
Cardiac markers are proteins that can be measured in your blood, urine or other bodily fluids. They can indicate damage to the heart muscle due to a heart attack (myocardial infarction) or other conditions such as inflammation or infection.
Cardiac markers are often used to help confirm a diagnosis of acute myocardial infarction (AMI). They may also be used for monitoring patients who have been treated with clot-busting medication or who have undergone coronary artery bypass surgery (CABG).
Myocardial infarction (MI) is a medical term used to describe a heart attack. A myocardial infarction occurs when blood flow to part of the heart is abruptly blocked, usually because of clotting within a coronary artery. A heart attack can cause damage to the heart muscle, which can lead to a loss of heart function.
The most common symptoms of cardiac marker rule out an MI include chest pain or discomfort and shortness of breath. Other symptoms may include pain or discomfort in the upper body, nausea and vomiting, sweating, lightheadedness or dizziness and fatigue.
Cardiac markers are substances that are released into your bloodstream when you have an MI. The three most commonly used cardiac markers are troponin T, troponin I and creatine kinase-MB (CK-MB).
What is an indicator of MI?
What is an indicator of MI?
Once the heart attack has been treated, the next step is to decide whether or not you have had a heart attack. The signs and symptoms are different for each person and may include:
Chest pain or pressure in your chest that lasts more than a few minutes, or goes away and comes back
Pain or discomfort in one or both arms, the back, neck or jaw
Nausea and vomiting
Sweating, especially at night
Shortness of breath with or without chest discomfort
Feeling like you might pass out