
Ultrasound İntussusception is the first-line imaging technique in the diagnosis and treatment of ileocolic intussusception. Most pediatric radiologists prefer to use ultrasound because it avoids radiation exposure, and can be performed rapidly at the bedside.
Ultrasound is more sensitive than plain radiography for detecting intussusception, but cannot reliably distinguish acute from chronic intussusception.
Ultrasound is a helpful modality for diagnosing and guiding therapeutic enema in the reduction of intussusception.
Ultrasound is a rapid imaging technique that does not require ionizing radiation. It is ideally suited for infants and small children. The technique can be used to identify intussusception, when the presence of an intraluminal mass or focal thickening of the wall is identified.
The role of ultrasound in the management of acute abdominal pain in children has been extensively studied. The sensitivity and specificity of ultrasound have been shown to be greater than 90% when used to diagnose intussusception.[5] Moreover, ultrasound is also useful in diagnosing other causes of acute abdominal pain, thus also reducing unnecessary surgeries.[6, 7] However, this technique may not be able to identify all cases of intussusception or cause; thus, surgical intervention may still be warranted in some cases.
The use of ultrasound is currently gaining popularity as a primary diagnostic modality for children presenting with acute abdominal pain. The effectiveness of ultrasound as a diagnostic tool for intussusception is well established.[8] Ultrasound can also be used for monitoring suspected cases during nonsurgical management and for detecting perforation when it occurs.[9]
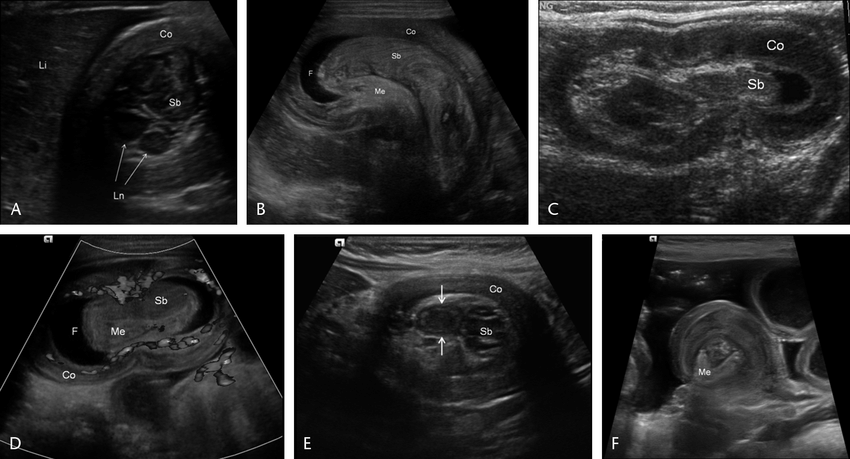
Ultrasound is used to confirm the presence of intussusception. Findings on ultrasound that suggest intussusception include an intestinal loop with a target appearance (ie, the distal end [apex] of the loop is echogenic and the proximal end [base] is hypoechoic). These findings are often described as double target sign or pseudokidney sign.
A positive sonographic finding for intussusception is the “target sign.” This sign represents bowel invaginated into itself, with a hyperechoic (bright) outer ring and a hypoechoic (dark) inner ring. Other sonographic findings include a “pseudokidney” appearance of the bowel, where there are concentric rings of alternating echogenicity, and a mesenteric mass containing fluid-filled loops of bowel
The classic finding on ultrasound examination is the target or doughnut sign. The target sign consists of concentric hypoechoic and hyperechoic circles surrounding a bright central echogenic dot representing the intussusceptum. The doughnut sign has been described as multiple concentric rings of alternating echogenicity that resemble the cross-section of a bagel
The classic ultrasound finding
This is an excellent image of intussusception in a dog. The intussusception (red arrows) is easily seen along with the leading point (green arrow). The small amount of air within the bowel is likely diagnostic for intussusception.
Ultrasound of a bowel segment showing the serosa as a black hyperechoic line (black arrows), and the parenchyma as brighter gray echogenic tissue between the hyperechoic serosal lines. Note the stranding from inflammation in the mesentery at the left side, which was caused by intestinal adhesions and pressure from the intussusception.
Intussusception is a condition in which the bowel folds into itself. This can cause an obstruction, or blockage, of the bowel.
An intussusception usually occurs in the small intestine, but can also occur in the large intestine (colon). Most intussusceptions occur in children between 3 months and 5 years of age.
The cause of intussusception is unknown, but it may be related to viral infections.
Symptoms of intussusception include abdominal pain and vomiting. The patient may pass blood and mucus in the stool (known as currant-jelly stool). There is often a history of several days of intermittent vomiting prior to presentation. Other symptoms may include abdominal tenderness and distention, fever, lethargy, poor feeding and diarrhea.
Diagnosis is made with ultrasound examination or barium enema x-ray. Treatment involves surgery or reduction by hydrostatic pressure (pushing on the bowel from outside).
Intussusception is a bowel problem (a condition in which part of the intestine has slid into an adjoining part) that usually occurs in children aged 3 months to 7 years. It can be a medical emergency.
If your child has intussusception, treatment is needed right away. If it’s not treated, intussusception can cause serious complications, including death.
Intussusception results when one segment of the intestine telescopes into an adjacent segment, trapping air or fluid and food in the space between. The telescoping effect causes swelling and sometimes cuts off blood supply to the trapped portion of the intestine.
Intussusception is most common in boys between ages 3 months and 7 years, although it can occur at any age. The cause of intussusception isn’t fully understood, but it may be related to viral infections or other conditions that cause swelling and irritation of the intestine (inflammation).
Can Intussusception Be Seen On Ultrasound?
Ultrasound is the most widely used imaging modality for evaluation of intussusception. It is noninvasive, inexpensive and available at the bedside. It has a sensitivity of approximately 95%. In cases where ultrasound cannot evaluate the entire bowel (eg, if patient is morbidly obese or there are overlying loops of bowel), CT may be appropriate.
Ultrasound should not be used to confirm reduction; rather, it can be used as a screening tool to see if reduction is complete.
The findings on abdominal ultrasound vary based on the duration of symptoms and stage of the intussusception. Early findings include nonspecific stomach distension or loss of normal pyloric-duodenal fluid with an echogenic mass in the right upper quadrant. With prolonged duration, lack of blood flow will lead to gut wall edema, which will appear as thickening of the bowel wall and loss of normal layering.
Intussusception is the telescoping of one segment of bowel into an adjacent segment. Intussusception can be seen on ultrasound as a target-like appearance, with alternating hyperechoic and hypoechoic layers. The hyperechoic layer represents the folded mucosa and submucosa of the leading edge of the intussusceptum, and the hypoechoic layer represents its mesentery, containing the blood vessels supplying the intussusceptum. The presence of edema in the leading edge of the intussusceptum produces a noncompressible ring sign.
Intussusception is most commonly seen in children aged 3 to 6 months. It typically involves the ileocecal junction or distal ileum, but it can involve any portion of bowel from duodenum to colon.
Ultrasound is a good way to diagnose intussusception. However, in some cases, the ultrasound may not show the problem. If your doctor thinks you have an intussusception and the ultrasound doesn’t show it, he or she may recommend a barium enema. This test shows pictures of your child’s intestine using X-rays and can confirm the diagnosis.
Intussusception occurs when one segment of the intestine telescopes into an adjacent segment. Intussusception most commonly occurs in children between the ages of 3 months to 6 years. However, it can occur at any age.
The causes of intussusception are not completely understood. In about 10%–25% of cases, a lead point is found that acts as a focus for the telescoping to occur. Lead points may be Meckel diverticulum or other intestinal duplication cysts, intestinal lymphoma, polyps, or inflammatory tissue from Crohn disease or Henoch-Schönlein purpura (HSP). The cause is idiopathic in about 75%–90% of cases.
An ultrasound can sometimes show intussusception but not always and I have been unable to find any statistics saying how often it is seen on ultrasound.
It is much more likely that the cause of the problem will be diagnosed with a CT scan than with an ultrasound.
Ultrasound is often useful in diagnosing intussusception. However, it is not always detectable by ultrasound. In this case, the doctor may order a barium enema or CT scan. This will allow them to see whether the intestine is telescoped into itself, as well as the location of the intussusception.
If intussusception is found, the treatment will depend on its severity and location. If it is in the upper region of the intestine and has not caused too much damage, it may be possible to push back (reduce) the distended intestine with an air or liquid enema
Intussusception occurs when a portion of the intestine telescopes into a more proximal segment. It most commonly occurs in children between the ages of 3 months and 6 years but can affect adults as well. Intussusception is caused by viral gastroenteritis in children and malignancy or lymphoma in adults.
The hallmark of intussusception is a sausage-shaped mass on ultrasonography, computed tomography (CT), or barium enema.
On ultrasound, intussusception is seen as multiple concentric layers of varying echogenicity that rotate around a single axis (see the first 2 images below). The interior wall often has an appearance similar to a target sign. If the intussusception is not reduced, bowel distention and air-fluid levels may be observed (see the image below).
If untreated, intussusception can lead to intestinal necrosis and perforation. The mortality rate from intestinal perforation alone is 20%. The mortality rate for patients who undergo surgery for complications associated with intussusception is about 1%.
Intussusception is a condition of the gastro-intestinal tract (GIT). It occurs when one part of the GIT slides into itself like a telescope, causing an obstruction. It can be seen in children and adults, although it is more common in children. Ultrasound may be used to diagnose intussusception and guide treatment.
What is intussusception?
The normal GIT has many folds. The small intestine is located towards the right side and lower abdomen and the large intestine is located on the left side and lower abdomen. These folds allow muscles of the abdomen to work efficiently to move food through the GIT. The oesophagus, stomach, small intestine and large intestine (colon) all connect together like beads on a necklace.
Can Intussusception Be Missed On Ultrasound?

Intussusception is a common problem in children and can be missed on ultrasound. A study published in the Journal of Ultrasound in Medicine looked at the accuracy of ultrasound in diagnosing intussusception.
The diagnosis of intussusception on ultrasound is made when visualization of a target lesion with an inner hyperechoic ring, an outer hypoechoic ring, and a central echolucent area is seen. The target lesion may not be present at the time of imaging because it can be intermittent or transient. Without seeing the target lesion, the diagnosis of intussusception can be missed if there are other nonspecific findings such as ileus or edema.
In this study, ultrasound was performed before enema for children with suspected intussusception. If ultrasound was negative but the clinical suspicion for intussusception was high, enema was then performed. In this series, enemas were successful in reducing intussusception in 27 of 29 patients (93%). Of these 27 patients, 14 had normal ultrasounds prior to enema and 13 had abnormal ultrasounds. Sensitivity and specificity for detecting intussusception by ultrasound alone were 44% and 100%.
This means that when
The majority of intussusceptions are ileocolic, with the ascending colon as the most common location for the lead point. Intussusception can be missed on ultrasound, but it’s difficult to miss the typical signs of intussusception.
Sonographic findings of intussusception include:
The target sign: a hypoechogenic center with hyperechogenic concentric rings (the “bullseye” sign). It is thought that this occurs from mucosal edema and hemorrhage surrounding the invaginated bowel.
A visible lead point, which is usually a mass or lymphnode
Peristaltic waves in normal colon proximal to the lesion
Incomplete encasement of the affected segment by an echogenic band, known as a pseudokidney sign. This occurs when only part of the circumference of the colon has been invaginated. The remainder of bowel wall shows normal peristalsis
Intussusception can be missed on any diagnostic method. The overall accuracy of US for intussusception is approximately 75-80% with the highest accuracy noted in the clinic setting.
The other imaging modalities that have been used to diagnose intussusception include air enema, barium enema and CT enteroclysis.
Air enema is a relatively safe procedure with a complication rate of less than 1% with more than 90% success rate in reducing intussusception. The disadvantage of this method is that it has a high likelihood of missing the intussusception if it is located proximal to the ileocecal valve.
Barium enema is similar to air enema in terms of its complication profile but has similar pitfalls associated with air enema. Barium used to be the mainstay diagnostic and therapeutic modality for reduced intussusceptions but has fallen out of favor due to the risk of perforation, which can occur as high as 1:200 cases.
The intussusception was missed on ultrasound. Why? There is no fixed rule as to what can and cannot be seen on ultrasound. The survey is operator dependent. The best trained sonologists can miss finding a problem (yes, we are all human). In my experience, missed findings occur most often in obese patients or in the very young.
If you have further questions, I would suggest speaking with your pediatrician, or the radiologist who performed your child’s study. They will be able to review the images with you and let you know if anything was overlooked or not investigated thoroughly enough.
Although the accuracy of ultrasound is well known, there are still some important points to consider. The incidence of missed intussusception is reported to be 11%. This can be due to lack of experience, especially with the more subtle cases. However, an excellent technique and proper equipment are needed to diagnose this condition correctly. It is also very important to remember that although ultrasound is a sensitive and accurate method for diagnosing intussusception, it is not specific.
Intussusception should be considered as a possible diagnosis if there is a mass in the abdomen and bowel obstruction or colic. In intussusception, the patient may have bloody diarrhea or vomiting.
The sensitivity of ultrasound in detecting intussusception has been reported as 53% when performed by pediatricians; however, it increases to 100% when performed by radiologists.
A retrospective review of the imaging studies performed on 43 consecutive patients with surgically proven intussusception was undertaken to determine the sensitivity, specificity, and accuracy of ultrasound in detecting intussusception.
The ultrasound images were reviewed by three radiologists with experience in pediatric radiology. The clinical history and final diagnosis were not known to the radiologists who were asked to comment on whether or not intussusception was present and if so, its site and likelihood for reduction. The results were compared to those of surgical findings.
The sensitivity of ultrasound for detecting intussusception was 95%, specificity 81%, and accuracy 90%. In only two cases was the site of intussusception at variance with that found at surgery. In both these cases, there was a transition zone between normal-appearing small intestine and abnormal-appearing bowel immediately adjacent to the area where the small bowel narrowed. These areas appeared as a “shadow” in the small bowel lumen, which may have been erroneously interpreted as an intussusceptum.
Ultrasound examination is an accurate method for diagnosing intussusception. It can be used alone or in conjunction with other diagnostic techniques such as barium enema or air contrast examination to make a definitive diagnosis
The “target sign” is created when the intussusceptum (the portion of bowel within) has a leading edge of hyperechoic mucosa and mesentery, a hypoechoic lumen, and hyperechoic mesentery.
The “doughnut sign” is seen with a concentric ring of valvulae conniventes surrounding the intussuscipiens.
The “pseudokidney sign” is formed by two layers of bowel wall with an echo-free center. It results from the telescoping of an ileocecal valve into a more proximal segment of bowel.
Doppler ultrasonography can be used in addition to grey scale imaging to characterize vascularity within an intussusception. The normal hyperemia associated with a target lesion may be absent in cases where the intestine is necrotic due to infarction as a result of venous or arterial compromise.